Menu
Working to Achieve Nationally Standardized, Sensible Electronic Claiming and Coding for Home Infusion
Standardized electronic claiming and coding for home infusion is one of NHIA’s top priorities and our hard work on this important issue brought about a significant victory in 2001 when the federal government’s HCPCS administrators published national standardized coding for home infusion therapy services effective in January of 2002. Since then, the HCPCS per diem S-code system has been widely adopted by commercial payers and some government payers throughout the nation. These codes are compliant with federal Health Insurance Portability and Accountability Act (HIPAA) regulations that mandate that all public and private payers use “approved” standardized coding for all of their health care transactions.
To help payers and providers of home infusion services comply with these requirements, in January 2002 NHIA released its first version of the educational resource, the NHIA National Coding Standard for Home Infusion Claims Under HIPAA.
The 2024 NHIA National Coding Standard has been updated to include new home infusion service codes and changes to the description of existing codes. These changes were a result of NHIAs ongoing efforts to modernize the home infusion code set to reduce the need to utilize not otherwise classified (NOC) codes by expanding the code set to account for newer drug therapies that have come to market since the S-code set was first introduced 20+ years ago. Significant changes from the previous version are highlighted in red within the document.
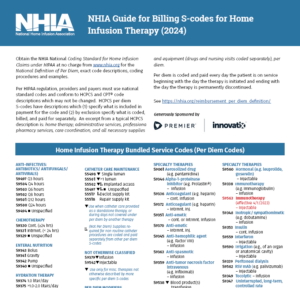
NHIA also offers three downloadable coding references to our members.
The standardization of pertinent and relevant definitions is inherently advantageous to all stakeholders within the health care delivery system. Such standardization reduces the chance of differing expectations amongst stakeholders, encourages benchmarking and analysis that is based upon comparable data sets, and generally fosters communication and cooperation between the various entities responsible for providing medically necessary health care services. With infusion therapy, reimbursement is often based upon a per diem approach, yet frequently this term is left undefined. Accordingly, as the national organization representing infusion services, the National Home Infusion Association (NHIA) presents the following definition of the term “per diem.”
As related to reimbursement, the term “per diem” represents each day that a given patient is provided access to a prescribed therapy, beginning with the day the therapy is initiated and ending with the day the therapy is permanently discontinued. The term “permanently” shall not be construed to infer that a therapy shall never again be initiated, but rather that continuation of the therapy is simply not predicted or anticipated at the time of cessation. The expected course and duration of the treatment shall be determined by the plan of care as prescribed by the ordering physician.
It shall not be necessary for the patient to receive an actual drug infusion each and every day in order to be considered covered under an existing per diem, so long as additional infusions are anticipated in the near future as prescribed in the physician plan of care. The fact that the health care provider anticipates continued responsibility for the patient and incurs costs related to such responsibilities, remains accountable for the provision of such anticipated care, and is responsible for the acquisition and allocation of resources that will be necessary to meet these obligations, shall deem the existing per diem to be current, valid, and in force.
This definition is valid for per diem therapies of duration of up to and including every 72 hours. Therapies provided beyond this range (weekly, monthly, etc.) fall outside of the per diem structure, and should have separate reimbursement rates that are specified on a contractual or other basis.
Examples: For purpose of demonstration, the following examples are provided:
Prescribed Therapy Units of Service Infusion every 4 hours for 14 days 14 Infusion every 8 hours for 14 days 14 Infusion every 12 hours for 14 days 14 Infusion every 24 hours for 14 days 14 Infusion every 48 hours for 14 days 14 Infusion every 72 hours for 14 days 14 Infusion once per week 1 (per week) Infusion once per month 1 (per month)
Costs associated with therapies that are of a more infrequent nature (72 hours, 48 hours, etc.) are less than those that are more frequent, and decreased reimbursement for such services is thereby appropriate. Using the above as an example, it is expected that the “Every 72 hours” per diem would be reimbursed at lesser daily rate than the “Every 4 hours” per diem, and that the units of service would remain identical.
Per diem reimbursement is intended to compensate for costs plus a fair return, i.e. the excess of revenues over expenses needed to ensure continued access to these therapies, for the following services, products and other support costs of an infusion therapy provider:
Dispensing
Medication profile set-up and drug utilization review
Monitoring for potential drug interactions
Sterile procedures including intravenous admixtures, clean room upkeep, vertical and horizontal laminar flow hood certification, and all other biomedical procedures necessary for a safe environment
USP-797 compliant sterile compounding of medications
Patient counseling as required under OBRA 1990
Clinical Monitoring
Development and implementation of pharmaceutical care plans
Pharmacokinetic dosing
Review and interpretation of patient test results
Recommending dosage or medication changes based on clinical findings
Initial and ongoing pharmacy patient assessment and clinical monitoring
Measurement of field nursing competency with subsequent education and training
Other professional and cognitive services as needed to clinically manage the patient pharmacy care
Care Coordination
Patient admittance services, including communication with other medical professionals, patient assessment, and opening of the medical record
Patient/caregiver educational activities, including providing training and patient education materials
Clinical coordination of infusion services care with physicians, nurses, patients, patient’s family, other providers, caregivers and case managers
Clinical coordination of non-infusion related services
Patient discharge services, including communication with other medical professionals and closing of the medical record
24 hours/day, 7 days/week availability for questions and/or problems of a dedicated infusion team consisting of pharmacist(s), nurse(s) and all other medical professionals responsible for clinical response, problem solving, trouble shooting, question answering, and other professional duties from pharmacy staff that do not require a patient visit
Development and monitoring of nursing care plans
Coordination, education, training and management of field nursing staff (or sub-contracted agencies)
Delivery of medication, supplies and equipment to patient’s home
Supplies and Equipment
DME (pumps, poles and accessories) for drug and nutrition administration
Equipment maintenance and repair (excluding patient owned equipment)
Short peripheral vascular access devices
Needles, gauze, non-implanted sterile tubing, catheters, dressing kits and other necessary supplies for the sale and effective administration of infusion, specialty drug and nutrition therapies
Multiple Categories of Pharmacy Professional Services
Maintaining comprehensive knowledge of vascular access systems
Continuing education to professional pharmacy staff
Removal, storage and disposal of infectious waste
Maintaining accreditation, including:
Maintaining the substantial insurance requirements (e.g. liability), including compliance with all state and federal regulations related to minimal insurance coverage
Administrative Services
Administering coordination of benefits with other insurers
Determining insurance coverage, including coverage for compliance with all state and federal regulations
Verification of insurance eligibility and extent of coverage
Obtaining certificate of medical necessity and other medical necessity documentation
Obtaining prior authorizations
Performing billing functions
Performing account collection activities
Internal and external auditing and other regulatory compliance activities
Retrieval and storage of medical and reimbursement records
Maintaining inventories of drugs, equipment, administration supplies and office supplies
Maintaining physical plant and offices, including building, equipment and furnishings, utilities, telephone, pagers, office supplies, etc.
Maintaining computer clinical and administrative information systems
Postage and shipping
Design and production of patient education materials
Quality assessment and improvement activities
Continuing education to administrative staff
Legal and accounting services
Licensing application activities and fees
Other Support Costs
Wages, salaries, benefits, payroll taxes, FICA, unemployment insurance, and workers compensation premiums
Property taxes
Asset depreciation
Inventory carrying costs
Accounts receivable carrying costs associated with carrying of large accounts receivable balances
Costs of insurance coverage per state regulations
Costs of maintaining accreditation (The Joint Commission, CHAP, ACHC, etc.)
New product research and development
Sales, advertising, and marketing
Community commitment and charitable donations
Cost of bad debt (uncollectible accounts receivable)
Other applicable overhead and operational expenses
Products and Services Not Included in the Definition of Per Diem
All drugs*, biologicals, enteral formulae and blood products
Nursing services provided directly to patients in their residences or other alternate sites
Other services provided directly to patients in their residences or other alternate sites by provider’s staff or representatives (e.g. dietician for nutritional counseling)
PICC and Midline insertion procedures and associated supplies
Surgically implanted central vascular access devices
Invasively placed digestive tract access devices for enteral therapy, including G tubes, NG tubes, J tubes, etc.
Services and products not considered part of the per diem compensation as may be agreed to by provider and payer (e.g. delivery to high risk areas with escort or extra protection, wound care supplies and devices for sites other than IV catheter insertion sites, etc.)
Services and products that may be provided at request of the patient that are considered by provider to be not medically necessary and beyond the scope of inclusion in the per diem
All services and products provided when not otherwise paid for through per diem coding for a therapy episode.
* Except that components which are part of a standard TPN formula are included in the per diem: (a) non-specialty amino acids (e.g., Aminosyn®, FreAmine®, Travasol®), (b) concentrated dextrose (e.g., D10, D20, D40, D50, D60, D70), (c) sterile water, (d) electrolytes (e.g., CaCl2, KCL, KPO4, MgSo4, NaAc, NaCl, NaPO4), (e) standard multi-trace element solutions (e.g., MTE4, MTE5, MTE7), and (f) standard multivitamin solutions (e.g., MVI-12 or MVI‑13). Excluded from per diem reimbursement and reimbursed separately are other drugs associated with TPN therapy: (a) specialty amino acids for renal failure (e.g.,Aminosyn-RF®, NephrAmine®), (b) specialty amino acids for hepatic failure (e.g., HepatAmine®, Hepatasol® 8%), (c) specialty amino acids for high stress conditions (e.g., Aminosyn-HBC®, BranchAmin®, FreAmine HBC®, Premasol®, TrophAmine®), (d) specialty amino acids with concentrations of 15% and above when medically necessary for fluid restricted patients (e.g., Aminosyn® 15%, Clinisol® 15%, Prosol® 20%), (e) lipids (e.g., Intralipid®, Liposyn®), (f) added trace elements not from a standard multi-trace element solution (e.g. chromium, copper, iodine, manganese, selenium, zinc), (g) added vitamins not from a standard multivitamin solution (e.g. folic acid, vitamin C, vitamin K), and (h) products serving non-nutritional purposes (e.g., heparin, insulin, L-Carnitine, iron dextran, Pepcid®, Sandostatin®, Zofran®). (Please note: trade names are used to provide a definition of per diem that communicates well; however, use of trade names is not a product recommendation or comment on extent of use in practice.)
Summary. As the national standardization of relevant and pertinent definitions is deemed inherently advantageous to all stakeholders; and as NHIA is the national organization representing infusion services and standards, it is hereby established that the preceding definition of the phrase “per diem” is the national standard for purposes associated with infusion therapy reimbursement.
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |